1. Iatrogenic Foreign Body(XA0056.mp4)
XA0056.mp4:SHA256:XXX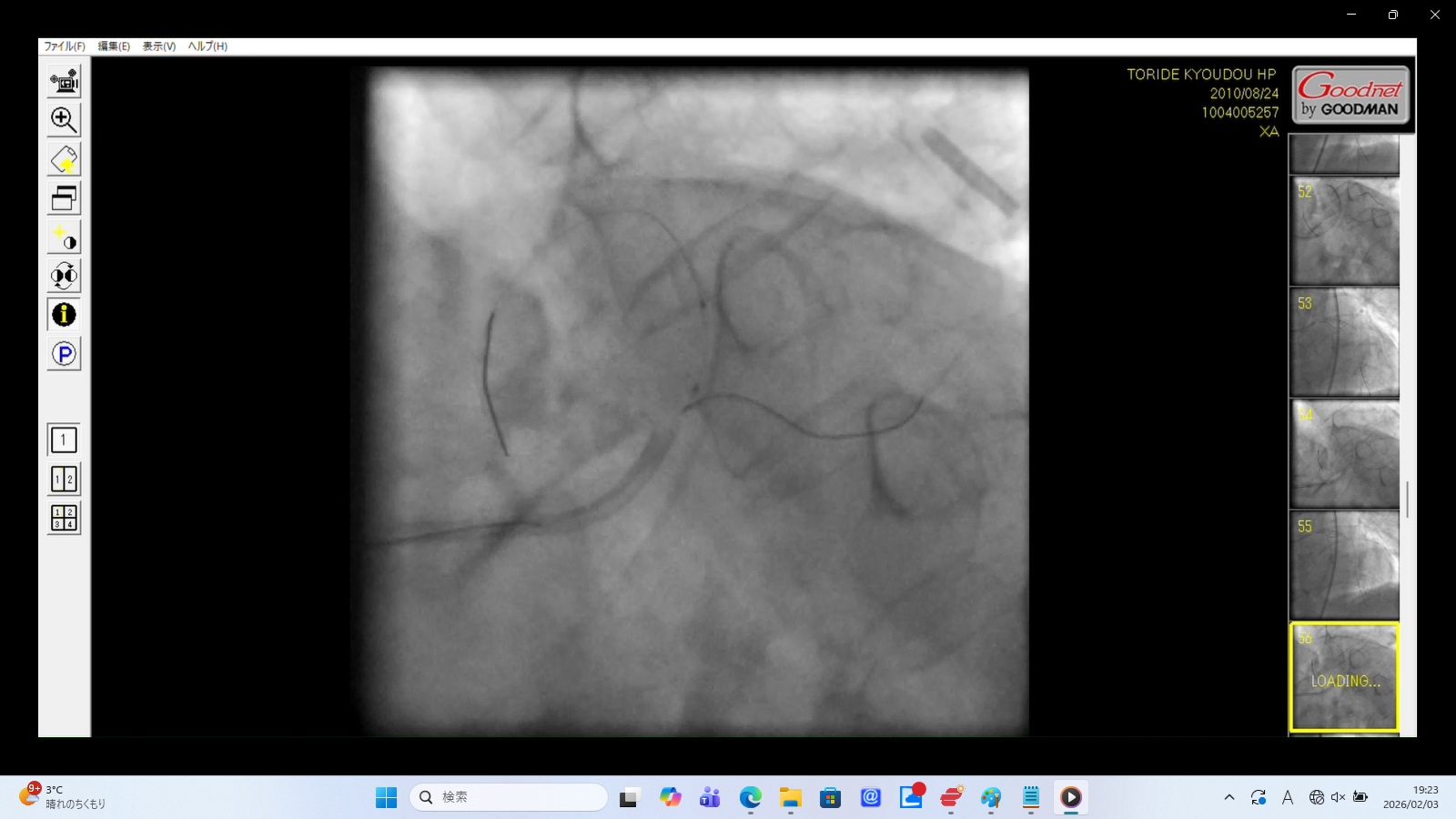
1. The Unidentified Foreign Body (The "Smoking Gun")
Caption: Evidence of Iatrogenic Foreign Body Displacement
Medical Findings:
Cylindrical Radio-opaque Object: A distinct, cylindrical metallic-density object is visible in the upper-right quadrant of the frame.
Synchronous Movement: The object moves rhythmically with the cardiac pulsation, indicating it is located within the thoracic cavity or pericardium.
Significance: This is an unaccounted-for medical device fragment (likely a detached catheter tip or stent). Its presence, combined with the lack of any mention in official medical records or the autopsy report, is irrefutable evidence of a surgical mishap followed by an institutional cover-up.
2. Iatrogenic Dissection(XA0020.mp4)
XA0020.mp4:SHA256:XXX
Finding: Contrast media flows abnormally slowly into the LAD, expanding in a non-anatomical fashion.
Interpretation: Strong evidence of coronary artery dissection. The catheter appears to be wedged in a false lumen, and the "slow flow" represents the physical peeling of the vessel wall layers in real-time.
3. LMT Structural Failure(XA0034.mp4)
XA0034.mp4:SHA256:XXX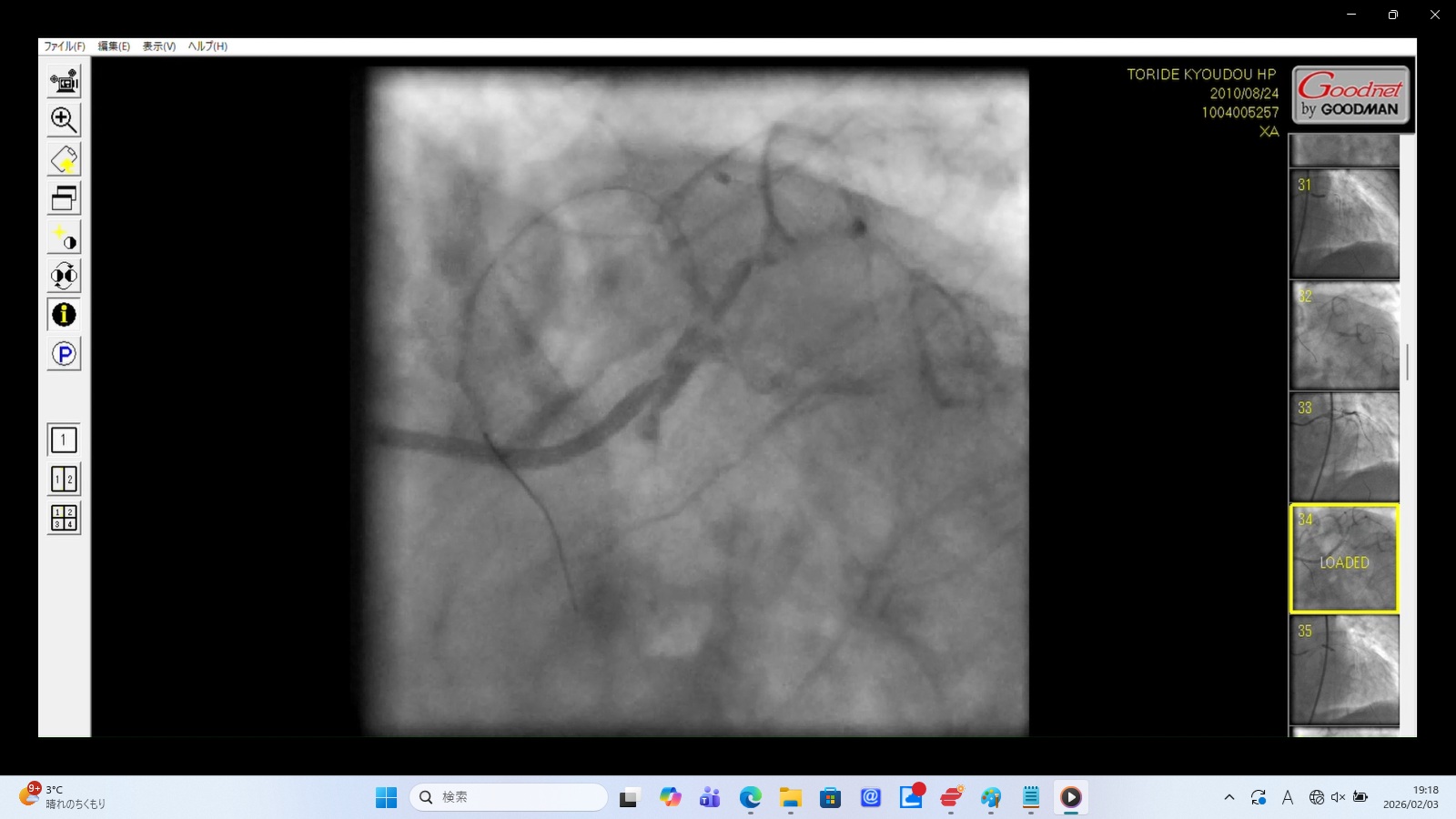
Finding: Presence of a false lumen within the Left Main Trunk (LMT) and direct leakage from the LMT into the exterior.
Interpretation: This confirms severe structural failure of the coronary artery. The LMT has been functionally destroyed, leading to both internal dissection and external hemorrhage.
4. LAD Perforation(XA0066.mp4, XA0072.mp4)
XA0066.mp4:SHA256:XXX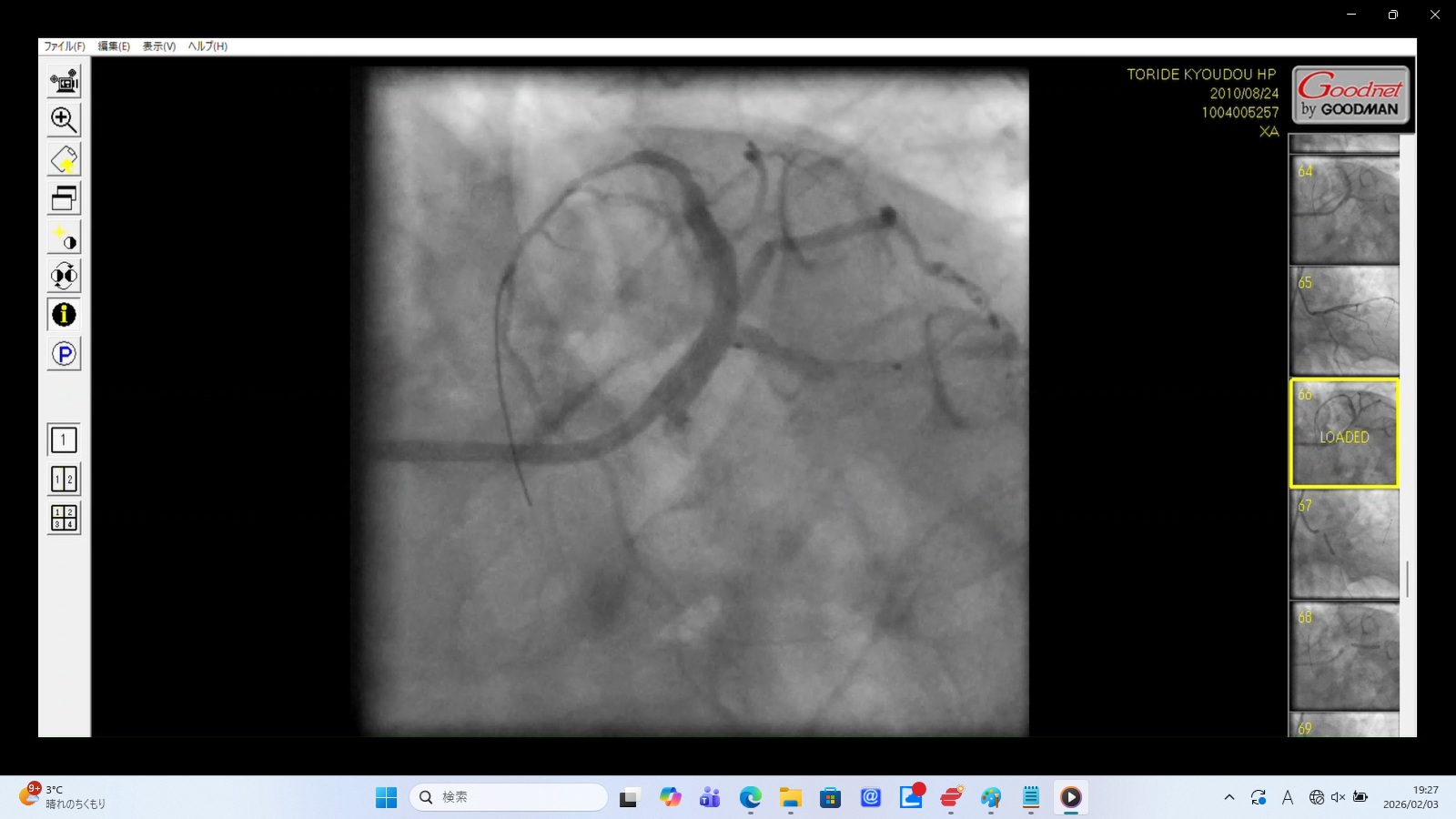
XA0072.mp4:SHA256:XXX

Caption: Evidence of Type III Coronary Perforation
Medical Findings:
Guidewire Deviation: The distal tip of the guidewire is clearly visible outside the anatomical boundaries of the LAD lumen.
Contrast Extravasation: Significant pooling of contrast media ("Staining") is observed in the pericardial space.
Significance: This is a catastrophic complication leading to rapid Cardiac Tamponade. The footage confirms a direct vascular injury that would require immediate surgical intervention or pericardiocentesis.
5. Diffuse Leakage(XA0019.mp4)
XA0019.mp4:SHA256:XXX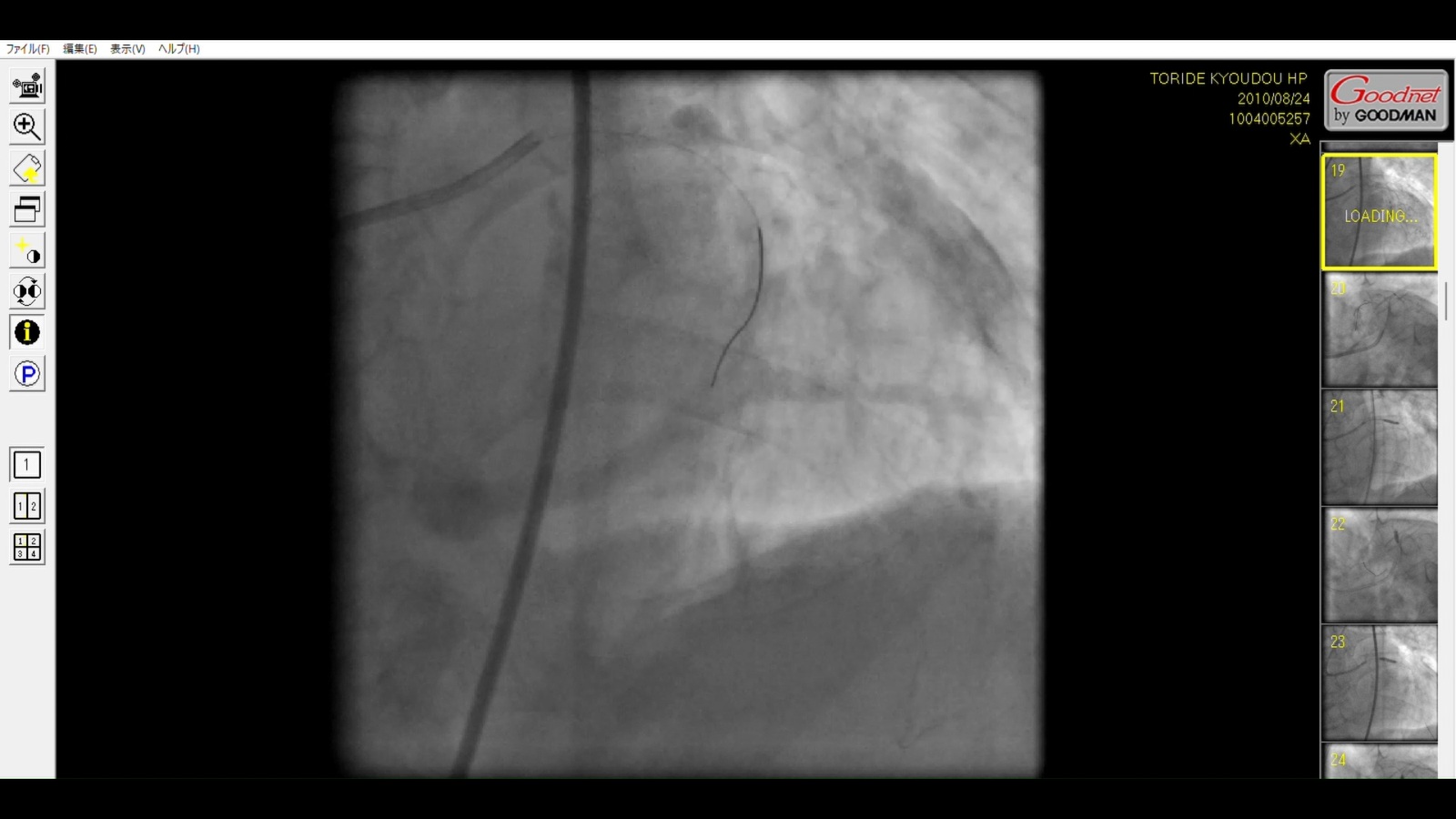
Finding: Pulsatile, cloudy movement of contrast media in the lower-left quadrant, independent of the injection timing.
Interpretation: This suggests contrast media and blood are leaking into the pericardial space, likely causing rapid cardiac tamponade.
6. Left Main Trunk (LMT) Total Occlusion(XA0082.mp4)
XA0082.mp4:SHA256:XXX
Caption: Iatrogenic Total Occlusion of the Left Main Trunk (LMT)
Medical Findings
Contrast Reflux: Upon injection, the contrast media fails to enter the coronary ostium and instead "bounces back" into the aortic root.
Suspected Dissection: The abrupt cessation of flow at the ostium suggests an iatrogenic dissection or mechanical collapse of the LMT.
Significance: This cuts off blood supply to approximately 75% of the myocardium. This is a periprocedural "Death Sentence" unless immediately bypassed.
Strategic Note: Deliberate Erasure of Critical Footage
Strategic Note: Deliberate Erasure of Critical Footage
•Gap 1 (27 Minutes): There is no video recorded between the official start time (22:35) and the first file (23:02), covering the period where the surgical approach was changed due to "failure."
•Gap 2 (18 Minutes): A critical 18-minute gap (23:08–23:26) exists exactly when medical records state "Distal Occlusion" and "Thrombectomy."
•Significance: The subsequent footage reveals a destroyed LMT and vascular perforation. The absence of video during the most high-risk maneuvers strongly suggests the intentional removal of incriminating evidence by the institution.
Physical Proof of Chain of Custody
Item: Photograph of the original CD-R provided through the evidence preservation process.
Markings: Clearly displays the names of "Toride Kyoudou Hospital" and the "Toride Police Station (Ibaraki Prefecture)."
Context: This confirms that the exact digital data (containing the fatal perforation and foreign body) was once seized by the police. The fact that the police returned this disk claiming "no findings" is a primary indicator of institutional complicity and the failure of the Japanese judicial system.